
Cranial Nerves and Swallowing
Cranial nerves important for swallowing include CN V (Trigeminal Nerve), VII (Facial Nerve), IX (Glossopharyngeal Nerve), X (Vagus), XI (Accessory Nerve) , and XII (Hyoglossus Nerve).
Sensory Innervation
Sensory receptors may respond to touch, flow, pressure, and taste (Steele & Miller, 2010). Sensory inputs for swallowing come from CN V, IX, and X. Taste is innervated by CN VII, IX, and X. Cranial nerve VII innervates taste in the anterior 2/3 of the tongue. CN IX innervates taste and sensory function in the the posterior 1/3 of the tongue. CN X innervates taste receptors in the epiglottis region.
Cranial Nerve V: Trigeminal
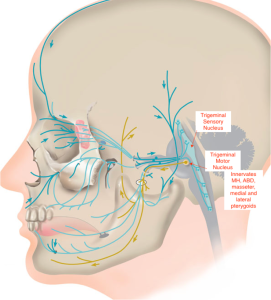
The mandibular branch of CN V provides sensory input for the anterior 2/3 of the tongue, the mucosa of the cheek, floor of mouth, gums (both upper and lower), temporomandibular joint, lower teeth, and the lower lip. Sensory input from the mucosa of the nasopharynx, soft palate, hard palate, gums, the upper teeth is transported through the maxillary branch. See Box 1.54 for a schematic of CN V.
Box 1.54: Cranial nerve V: Trigeminal
The trigeminal nerve is important for mastication and hyo-laryngeal trajectory.
Clinical Note
Damage to CN V may result in the following.
- Loss of oral sensation leads to reduced bolus control and awareness of bolus location.
- Damage to mandibular branch will reduce mastication skills.
- Reduced function in the floor of mouth (MH & ABD) muscles will reduce hyo-laryngeal trajectory, which may impact epiglottic down-folding and UES opening. The end result may be reduced airway protection during bolus passage in the pharynx, thus increasing the risk of laryngeal penetration. Also, increased risk of residue in either the vallecula or pyriform sinus leads to increased risk of penetration or aspiration after the swallow.
- Damage to tensor veli palatini may reduce velar-pharyngeal valving and lead to nasopharyngeal reflux of material.
Cranial Nerves IX and X: Glossopharyngeus & Vagus
CN IX provides sensory innervation to the posterior 1/3 of the tongue as well as the mucosa of the oropharynx, palatine tonsils, faucial pillars, and temporomandibular joint. The pharyngeal branch of CN X provides sensory innervation for the levator veli palatini muscle as well as the superior and middle pharyngeal constrictor muscles. The internal branch of the superior laryngeal nerve of CN X provides sensory innervation to the mucosa of the epiglottis, the supraglottic region, the laryngeal joint receptors, the aryepiglottic folds, and the posterior tongue. The recurrent laryngeal branch of CN X provides sensory innervation to the mucosa of the subglottic region and the esophagus. The esophageal branch of CN X provides sensory innervation to the esophageal mucosa and striated muscle in the esophagus. See Box 1.56 and 1.57 for schematics of CN IX and X, respectively.
Motor Innervation
Motor function for swallowing is innervated by CN V, VII, IX, X, XI, and XII.
Cranial Nerve V- Trigeminal
The mandibular branch of CN V innervates muscles of the jaw and soft palate (Box 1.54). The inferior alveolar branch of CN V innervates the mylohyoid and anterior belly of the digastric muscles. Muscles of the soft palate receive bilateral input from the cortex due to the bilateral upper motor neuron innervation of CN V. Therefore, asymmetrical movement implies a lower motor neuron lesion.
Cranial Nerve VII- Facial
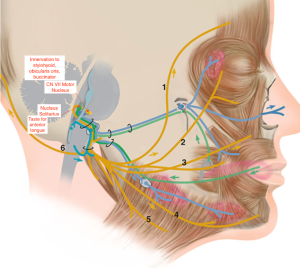
The facial nerve (CN VII) innervates both sides of the upper face, but only the contralateral side of the lower face (Box 1.55). In the lower face, the digastric branch of CN VII innervates the posterior belly of the digastric muscle. The buccal branch of CN VII innervates the orbicularis oris and the buccinator muscles. The stylohyoid branch of CN VII innervates the stylohyoid muscle.
Box 1.55: Cranial nerve VII: Facial
The facial nerve is important for taste, anterior containment, and oral bolus control.
Clinical Note
Damage to CN VII may result in the following.
- Reduced lip function may impact oral containment as evidenced by anterior spillage or drooling.
- Poor bolus control as evidenced by residue in buccal pockets.
- Reduced taste sensation in anterior tongue.
- Damage to secreto-motor systems may impact function of sublingual and submandibular glands, resulting in decreased oral saliva production.
Cranial Nerve IX, X, & XI: Glossopharyngeus, Vagus & Accessory
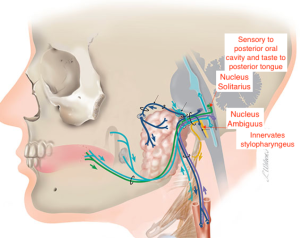
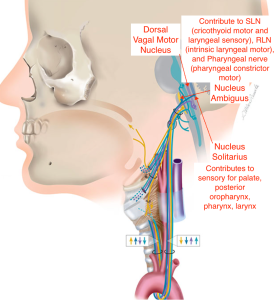
The muscular branch of CN IX innervates the stylopharyngeus muscle (Box 1.56). The cricopharyngeus muscle is innervated by CN X (Box 1.57). The recurrent branch of CN X (a.k.a. the recurrent laryngeal nerve) innervates all but one of the intrinsic laryngeal muscles including the thyroarytenoid, interarytenoid, lateral cricoarytenoid, and posterior cricoarytenoid muscles. It is also responsible for innervation of the thyroepiglottic muscle. The remaining intrinsic laryngeal muscle, the cricothyroid muscle, is innervated by the external superior branch of CN X.
Clinical Note
Damage to CN X may result in the following.
- Damage to innervation of intrinsic laryngeal muscles may reduce laryngeal valving leading to increased risk for aspiration during the swallow.
- Reduced sensory function to the pharynx and larynx may result in reduced reflexive cough response or weak cough reducing laryngeal clearance skills and increasing the risk of aspiration. It may also increase pharyngeal residue thereby increasing the risk of aspiration after the swallow.
- Impaired UES opening resulting in pyriform sinus residue.
- Damage to innervation of pharyngeal constrictor muscles (shared with CN IX) may reduce pharyngeal compression leading to reductions in pharyngeal pressure, which may result in distributed pharyngeal residue.
- Reduced innervation to levator veli palatine muscle may reduce velar valving and lead to nasopharyngeal reflux or poor posterior oral containment.
The pharyngeal plexus, which contains fibers from CN IX and X (and likely some fibers from CN XI), innervates the muscles of the anterior and posterior faucial pillar, the palatopharyngeus and palatoglossus muscles, the salpingopharyngeus muscle, and the three pharyngeal constrictor muscles —SPC, MPC, and IPC. Fibers from CN X and XI innervate the levator veli palatine and uvular muscle. Damage to the pharyngeal plexus will impair pharyngeal shortening and reduce pharyngeal motility. Cranial nerve XI innervates the palatoglossus muscle.
Box 1.56: Cranial nerve IX: Glossopharyngeal
The glossopharyngeal nerve is important in the swallow trigger. It also contributes to pharyngeal compression.
Clinical Note
Damage to CN IX may result in the following.
- Reduced sensation of posterior tongue and oropharynx which may alter taste and reduce trigger response time (delayed or absent).
- Damage to innervation of pharyngeal constrictor muscles (shared with CN X) may reduce pharyngeal compression leading to reductions in pharyngeal pressure, which may result in distributed residue.
- Damage to innervation the of stylopharynges muscle may result in reduced pharyngeal shortening.
- Reduced gag reflex.
- Reduced posterior oral sensation may lead to poor oral posterior containment resulting in premature spillage and increasing the risk of penetration and aspiration before the swallow.
Box 1.57: Cranial nerve X: Vagus
The vagus nerve is important for swallow safety and pharyngeal compression.
Cranial Nerve XII: Hyoglossus
Cranial nerve XII innervates all the intrinsic and extrinsic tongue muscles. The geniohyoid muscle is innervated by the ansa cervicalis, which contains nerve fibers not only from CN XII, but also cervical spinal nerve C1. The thyrohyoid muscle, a supraglottic muscle is also innervated by CN XII.
Just for Fun
Click here to see a fun way to learn and remember the innervation of the tongue.
Clinical Note
Damage to CN XII may result in the following.
- Reduced innervation to intrinsic and extrinsic muscles on the tongue may lead to poor bolus control in the oral cavity leading to reduced mastication and potential residue in oral spaces after the swallow. It may also result in premature spillage.
- Reduced base of tongue to posterior pharyngeal wall contact may lead to reduced driving pressure on the bolus, which may result in slowed transit, inadequate UES opening, and pharyngeal residue.
If on protrusion, the tongue deviates to one side, consider either hypoglossal nerve injury on the side of the tongue deviation, or a cortical lesion on the contralateral side. When noted, inspect the tongue for unilateral atrophy. An individual who recently suffered from a stroke is less likely to present with unilateral tongue atrophy. Yet, atrophy is often noted with hypoglossal nerve injury (Blondin et al., 2011).
