Impact of Cranial Nerve Damage on Swallow Function
Impact of Cranial Nerve Damage on Swallow Function
In chapter 1, the impact of CN damage was briefly addressed and is reviewed here. Injury to the sensory and motor innervation pathways can result in deficits in feeding or swallowing especially when cranial nerves V, VII, IX, X, XI, or XII are involved. Understanding the role of these cranial nerves allows you to anticipate the impact that CN damage will have on swallow function. In a focal injury, swallow function will be altered in a predictable pattern depending on the location and extent of the damage. Box 2.29 through 2.34 schematically indicate risks to swallow physiology in the event of cranial nerve damage.
CN V: Trigeminal Nerve
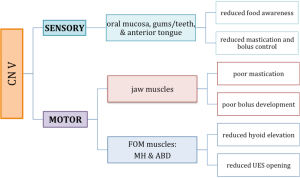
CN V carries sensory function to the oral cavity and motor function to jaw and floor of mouth muscles. Damage to this nerve may result in reduced awareness of oral bolus, which can lead to poor bolus control, oral residue or/and reduced mastication. It also impacts hyo-laryngeal trajectory thereby altering UES opening (Box 2.29).
Box 2.29: CN V and associated impact on swallow function if damaged
CN VII: Facial Nerve
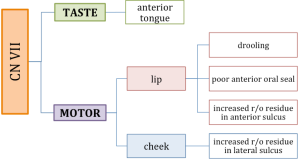
CN VII carries sensory fibers for taste to the anterior tongue and motor fibers to the lips and cheek region. Damage to this nerve may result in (a) reduced taste perception for foods and liquids in the anterior oral cavity, (b) reduced lip motor function which may impact anterior oral containment, and (c) reduced buccal contraction yielding reduction in oral pressure and bolus control (Box 2.30). The latter may yield leakage into the oral lateral sulci. Damage to CN VII may also impact function of submandibular glands resulting in reduced saliva production, which may lead to difficulty in generating a cohesively formed bolus. Reduced saliva production is also implicated in tooth decay and increased oral bacteria.
Box 2.30: CN VII and associated impact on swallow function if damaged
Clinical Note
Damage to CN VII may result in the following.
- Reduced lip function may impact oral containment as evidenced by anterior spillage or drooling.
- Poor bolus control as evidenced by residue in buccal pockets.
- Reduced taste sensation in anterior tongue.
- Damage to secreto-motor systems may impact function of sublingual and submandibular glands and decreased oral saliva production.
CN IX, X & XI: Glossopharyngeal, Vagus, & Accessory Nerves
Although this text defines activities specific to each cranial nerve, in reality fibers from CNs IX, X, and XI combine at various points in the nerve’s journey. However, for simplicity, the damage profiles are presented per cranial nerve.
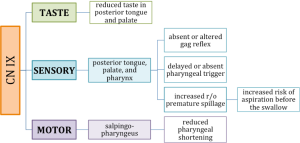
CN IX carries sensory, taste and motor fibers important for swallowing (Box 2.31). Taste fibers innervate the posterior tongue and palate. Therefore, damage to this CN may alter taste perception. Damage to this nerve may also result in reduced sensory function in the posterior oral cavity and pharynx, which may impact swallow trigger response or alter bolus control as it traverses from the horizontal to the vertical trajectory. It may also alter gag reflex response. Motor fibers from CN IX innervates the salpingopharyngeus muscle which is important in pharyngeal shortening. When damaged, reduced shortening will impact swallow timing and increase swallow safety risks.
Box 2.31: CN IX and associated impact on swallow function if damaged
Clinical Note
In summary, damage to CN IX may result in the following.
- Reduced sensation of posterior tongue and oropharynx which may alter taste and trigger response time (delayed or absent).
- Damage to innervation of pharyngeal constrictor muscles (shared with CN X) may reduce pharyngeal compression leading to reductions in pharyngeal pressure, which may result in distributed residue.
- Damage to innervation of stylopharyngess may result in reduced pharyngeal shortening.
- Reduced gag reflex.
- Reduced posterior oral sensation may lead to poor posterior containment resulting in premature spillage and increasing the risk of penetration and aspiration before the swallow.
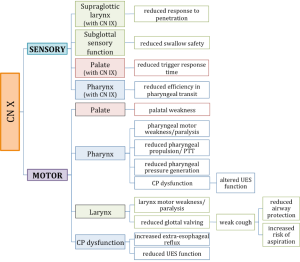
CN X (along with CN IX) provides sensory fibers to the palate, pharynx and larynx. Damage to this sensory system will impact both swallow safety and efficiency (Box 2.32). Airway protection may be reduced because penetrated material will not be reported by the sensory system and may be allowed to continue downward. Motor fibers innervate all intrinsic laryngeal muscles and pharyngeal muscles. When damaged, laryngeal valving may be inadequate to protect the airway. Pharyngeal constriction may be inadequate to aid in efficient propulsion of food through the pharynx.
Box 2.32: CN X and associated impact on swallow function if damaged
Clinical Note
Damage to CN X may result in the following.
- Damage to innervation of intrinsic laryngeal muscles may reduce laryngeal valving leading to increased risk for aspiration during the swallow.
- Reduced sensory function to pharynx and larynx may result in reduced reflexive cough response or weak cough reducing laryngeal clearance skills and increasing the risk of aspiration. It may also increase pharyngeal residue thereby increasing the risk of aspiration after the swallow.
- Damage to innervation of pharyngeal constrictor muscles (shared with CN IX) may reduce pharyngeal compression leading to reductions in pharyngeal pressure, which may result in distributed residue.
- Reduced innervation to lever veli palatine may reduced velar valving and lead to nasopharyngeal reflux or poor posterior oral containment.
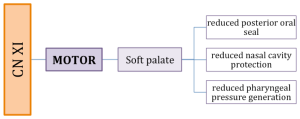
CN XI is a motor nerve that is involved in innervation of the velopharyngeal mechanism. Damage to this nerve may reduce the effectiveness of the nasopharyngeal closure and allow for leakage into the nasal cavity (Box 2.33).
Box 2.33: CN XI and associated impact on swallow function if damaged
CN XII: Hyoglossus Nerve
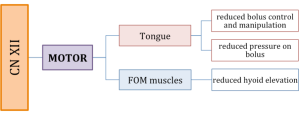
CN XII is a motor nerve that primarily innervates the tongue. Damage to this nerve may impact oral bolus control and formation. Further, reduced oral pressure generation resulting from a weakened tongue will reduce pharyngeal driving pressure, particularly if the base of tongue weakness is limited in its retraction (Box 2.34).
Box 2.34: CN XII and associated impact on swallow function if damaged